Golf Southwest - Course Reviews, Tips, & Other Golf Resources
Read our golf course reviews, discover new golf tips, and learn how to play fantasy golf and bet on golf!


Putting backspin on the ball, Hitting a lob wedge – Ask the PGA Pro – Junior Golfers #1
Ask the PGA Professional #2
Tailored clubs, How to figure out a handicap – Ask the PGA Professional #9

The Best Lesson I Ever Had
by Tom Ward As a golf instructor, I have been fortunate enough to travel extensively around the world teaching and developing golf programs in foreign lands to players from all walks of life. Over the years I have encountered numerous excuses from golfers on why they...

Achieving a Steady Head
Bunker shots, Relieving pressure – Ask the PGA Pro – Junior Golfers #17
Etiquette on the greens, How to hit a driver – Ask the PGA Pro – Junior Golfers #18
Going to Q School, Bunker shot advice – Ask the PGA Pro – Junior Golfers #21
Increasing driver yardage, hitting behind the ball – Ask the PGA Professional #13
Forward press, Keeping composure – Ask the PGA Professional #1
Going to College for Golf, New driver? Ask the PGA Pro – Junior Golfers #11
Coming over the top, Competing in golf – Ask the PGA Pro – Junior Golfers #9
Keep up to date with the golf world at Golf Magazine.

Mill Creek Golf & Country Club – Salado, TX

Texas Star Golf Course – Euless, TX

Tangle Ridge Golf Club – Grand Prairie, TX

Turtle Hill Golf Course – Muenster, TX

The Courses at Watters Creek – Plano, TX

The River Course at Keystone – Summit Country, CO

The Building of Turtle Hill Golf Course
Bridlewood Golf Club – Flower Mound, TX

Barton Creek Resort & Country Club – Austin, TX
More Golf Articles
Golf advice, exercise, stretching, book reviews and more.
Short Game Shots
Swing Fundamentals – Junior Golf Tips
Golfers, Don’t Fear the Irons
DraftKings Free Entry Ticket Promotion

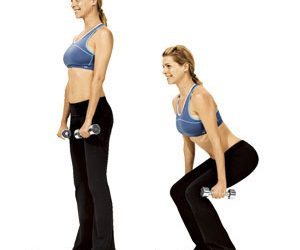
Tune Up, Tone Up, Warm up for Spring
Golf Rules – Provisional ball

What Your Golf Game Reveals About Your Personality
Golf Strategy & Mental Game

FanDuel Free Deposit Bonus Promotion
Golfing in the American Southwest
Golf in the American Southwest is as much a part of the culture as cowboy boots and barbeque. With stunning, sun-soaked landscapes, dramatic desert backdrops, and meticulous courses, the Southwest has firmly established itself as a premier golfing destination.
Golfing Galore in the Grand Canyon State
Arizona, often referred to as the Grand Canyon State, is a veritable golfer’s paradise. Home to more than 300 golf courses, it is famed for its illustrious golfing communities, particularly in areas like Scottsdale and Phoenix. The state boasts numerous championship courses designed by golfing legends and renowned architects.
The TPC Scottsdale, host to the Waste Management Phoenix Open, offers two stunning PGA Tour caliber courses. And then there’s the iconic Stadium Course, known for its thrilling 16th hole, possibly the most famous par-3 hole in all of golf.
Tucson is another golf haven within Arizona, where you can find the Omni Tucson National Resort, which has hosted more than 30 PGA Tour events.
New Mexico: High Desert Golfing
Next door, in New Mexico, golfers can tee off amidst landscapes that seem straight out of a painting. The state’s high altitude can add considerable distance to your drives, which makes for an exciting adjustment to your game.
One standout is the Paa-Ko Ridge Golf Club in Sandia Park, ranked one of the best public courses in the country. Its 27 holes offer breathtaking high desert views. Similarly, the Twin Warriors Golf Club at the Hyatt Regency Tamaya Resort offers a course intertwined with cultural and historical sites.
Nevada: From Vegas to the Valley
Nevada, while famous for its glitzy casinos, also holds its own in the golfing world. From Las Vegas to Reno, the state offers an array of courses for every level. In Vegas, the Shadow Creek Golf Course stands out with its exclusive, high-end experience. For stunning mountain and desert views, golfers can visit Wolf Creek in Mesquite.
Golfing in the Southwest isn’t just about playing a round; it’s about immersing yourself in the awe-inspiring landscapes that make each hole an adventure. The region blends the spirit of the sport with its distinct cultural charm and spectacular natural beauty, promising a unique golfing experience that goes beyond the fairways.
Remember, golf is as much a mental game as it is physical, and in the tranquil expanses of the Southwest, you’ll find a perfect environment to calm your mind, sharpen your focus, and truly play your best game!
Contact Us!
Thank you for visiting GolfSW.com. If you would like to reach us, please visit our contact form.